
Authors.
Christian S Marchello 1,✉, Samuel D Carr 1, John A Crump 1.
Copyright and License information
PMCID: PMC7695120 PMID: 32996447.
Abstract.
Understanding patterns and trends of antimicrobial resistance (AMR) in Salmonella Typhi can guide empiric treatment recommendations and contribute to country decisions about typhoid conjugate vaccine (TCV) introduction. We systematically reviewed PubMed and Web of Science for articles reporting the proportion of Salmonella Typhi isolates resistant to individual antimicrobials worldwide from any time period. Isolates resistant to chloramphenicol, ampicillin, and trimethoprim–sulfamethoxazole were classified as multidrug resistant (MDR), and isolates that were MDR plus resistant to a fluoroquinolone and a third-generation cephalosporin were extensively drug resistant (XDR). Among the 198 articles eligible for analysis, a total of 55,459 Salmonella Typhi isolates were tested for AMR (median 80; range 2–5,191 per study). Of isolates from 2015 through 2018 in Asia, 1,638 (32.6%) of 5,032 were MDR, 167 (5.7%) of 2,914 were resistant to third-generation cephalosporins, and 148 (8.3%) of 1,777 were resistant to azithromycin. Two studies from Pakistan reported 14 (2.6%) of 546 isolates were XDR. In Africa, the median proportion of Salmonella Typhi isolates that were MDR increased each consecutive decade from 1990 to 1999 through 2010 to 2018. Salmonella Typhi has developed resistance to an increasing number of antimicrobial classes in Asia, where XDR Salmonella Typhi is now a major threat, whereas MDR has expanded in Africa. We suggest continued and increased surveillance is warranted to inform empiric treatment decisions and that AMR data be incorporated into country decisions on TCV introduction.
INTRODUCTION.
Typhoid fever is a systemic infection caused by the bacterium Salmonella enterica subspecies enterica serovar Typhi (Salmonella Typhi) and is an important cause of illness and death worldwide, with an estimated 10.9 million new infections and 116,800 typhoid fever–related deaths occurring annually.1–3 Typhoid fever is difficult to distinguish from other causes of febrile illnesses, compounded by limited laboratory services in some low- and middle-income countries, making specific diagnosis and appropriate antimicrobial treatment challenging in routine practice.4–6
Historically, chloramphenicol, ampicillin, and trimethoprim–sulfamethoxazole were the first-line antimicrobial treatments for typhoid fever.7 However, multidrug resistant (MDR) Salmonella Typhi, defined as resistance to these three first-line drugs,8 was widespread by the late 1980s and 1990s, with reports from Pakistan, India, and other southern and Southeast Asian countries.9 Subsequently, ciprofloxacin became the drug of choice, but resistance appeared quickly, first in 199110 and in an outbreak in 1997.11 With the emergence of MDR Salmonella Typhi and MDR with fluoroquinolone resistance, third-generation cephalosporins, macrolides, and carbapenems have been used increasingly for the treatment of typhoid fever.7 Extensively drug resistant (XDR) Salmonella Typhi, defined as resistance to first-line antimicrobials, a fluoroquinolone, and a third-generation cephalosporin,12 was reported in Hyderabad, Pakistan, in 2016.13 Since then, the WHO has been notified of more than 10,365 infections with XDR Salmonella Typhi in Pakistan,14 and travel-associated infections have been reported in Canada,15 Denmark,16 Australia,17 and the United States.18 Hence, antimicrobial resistance (AMR) in Salmonella Typhi is a global threat.
Increasing access to safe drinking water, food, and improved sanitation are important measures for controlling the impact and spread of typhoid fever,19–21 but have elsewhere been associated with socioeconomic progress that has taken place over long time periods.22–24 Typhoid vaccines represent an important and accessible tool to avert illness and death in the short- to medium-term while water, food, and sanitation improvements take place. To assist countries with decision-making about typhoid conjugate vaccine (TCV) introduction and other control efforts, and to guide empiric management decisions for typhoid fever, we performed a comprehensive, systematic review of the literature to describe the prevalence and trends of AMR among Salmonella Typhi.
METHODS.
Search strategy and study selection.
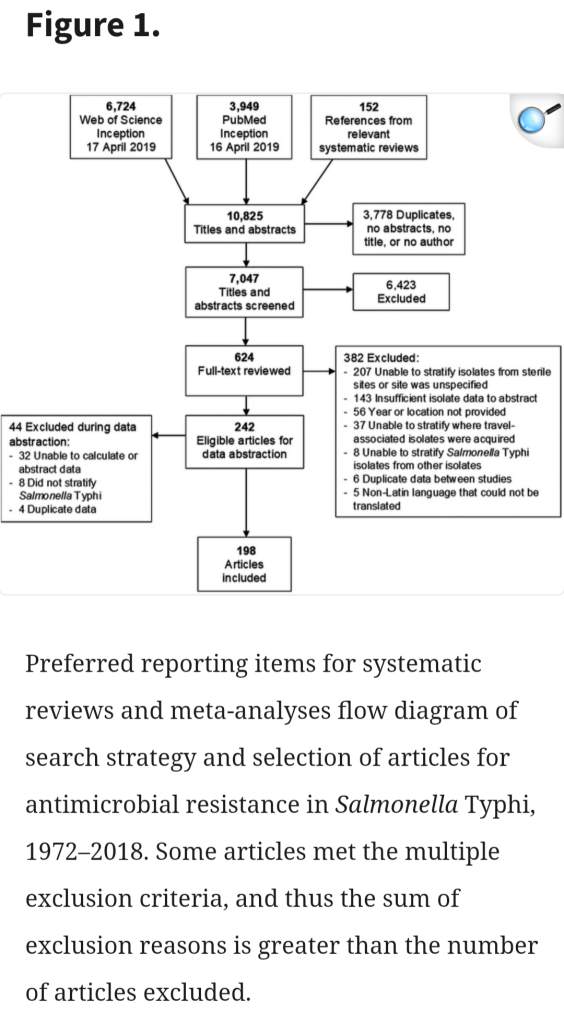
The systematic review protocol was registered with PROPSERO: International Prospective Register of Systematic Reviews (CRD42019131038) on May 10, 2019. Following the preferred reporting items for systematic reviews and meta-analyses,25 we searched two databases, PubMed from inception through April 16, 2019, and Web of Science from inception through April 17, 2019. Each search included key words of Typhi, typhoid, “enteric fever,” antimicrobial, susceptibility, and resistance (Supplemental Table S1). No restrictions were placed on location, date of specimen collection, or language of publication.
Epidemiologic studies of any design reporting antimicrobial susceptibility testing (AST) results of Salmonella Typhi isolated from human source, normally sterile site (e.g., blood, bone marrow) specimens, were included. Policy reports, commentaries, editorials, and conference abstracts were excluded, as were studies where we could not distinguish between isolates from normally sterile site specimens and isolates not from normally sterile site specimens (e.g., stool, urine). Studies that did not present sufficient detail to calculate the prevalence of AMR among all reported Salmonella Typhi isolates were also excluded. Studies reporting travel-associated infections were included only if we were able to identify the country where the infection was likely acquired.
Search results from each database were imported into Endnote X8 (Clarivate Analytics, Boston, MA). We also included studies identified from the reference lists of three previous reviews on bloodstream infections that also reported AST of Salmonella Typhi.26–28 Endnote was used to remove duplicates before a de-duplicated list of articles was uploaded to the online systematic review tool Rayyan (Qatar Computing Research Institute, Doha, Qatar).29 All subsequent processes were performed in parallel by two authors (C. S. M. and S. D. C.). We screened titles and abstracts for inclusion, and any article selected by at least one author was included for full-text review. We then screened each full-text article for inclusion, with discrepancies resolved through discussion or the involvement of a third author (J. A. C.). After establishing a final list of included full-text articles, two authors abstracted study characteristics and AST data in parallel using a shared Google Sheets spreadsheet (Google LLC, Mountain View, CA).
Data abstraction.
Study characteristics that were abstracted included first author, publication year, normally sterile specimen type, and country of specimen collection. When a study collected isolates from multiple locations within a country or in separate countries, we documented the additional locations as study sites. We abstracted data for the year of susceptibility testing; antimicrobial susceptibility testing (AST) interpretive criteria used, such as the Clinical and Laboratory Standards Institute (CLSI) or European Committee on AST, and year of criteria; AST method (e.g., agar dilution, disk diffusion); number of total isolates tested; and number of isolates that tested susceptible, intermediate, or resistant to a predefined list of antimicrobials. The predefined list was compiled from the CLSI M100 table of suggested antimicrobial agents for Enterobacteriaceae groups A and B.30 Because zone sizes or minimum inhibitory concentration (MIC) values were often not reported, we were unable to attempt to recategorize AST results for fluoroquinolones, third-generation cephalosporins, and azalides for the current CLSI interpretive criteria.31
In addition to recording susceptibility results to individual antimicrobials, data were also abstracted on the MDR phenotype, defined as resistance to chloramphenicol, ampicillin, and trimethoprim–sulfamethoxazole9; and the XDR phenotype, defined as resistance to ampicillin, chloramphenicol, trimethoprim–sulfamethoxazole, a fluoroquinolone, and a third-generation cephalosporin.12 Fluoroquinolones abstracted were ciprofloxacin or ofloxacin, and third-generation cephalosporins were ceftriaxone or cefotaxime. We subsequently classified study sites by UN geographic regions and subregions.
Analyses.
For each antimicrobial tested, we divided the number of resistant isolates by the total number of isolates tested and multiplied the resulting fraction by 100 to produce the proportion (%) of resistant isolates. When only the number of susceptible isolates was supplied and resistant isolates were not explicitly provided, we assumed that non-susceptible isolates were resistant. For example, an article described 90.0% of 100 isolates were susceptible to ampicillin, and we imputed data that 10 isolates in that study were resistant. No other data were imputed. Median proportions of isolates resistant by UN region and the chi-squared test for trend in proportions over four time periods (1970–1989, 1990–1999, 2000–2009, and 2010–2018) were calculated in R version 3.6.1 (R Foundation for Statistical Computing, Vienna, Austria). Time periods were selected by decade, combining the 1970s and 1980s because of limited data available during those years. Time series histograms using 5-year interval periods were produced in Microsoft Excel 2016 (Microsoft Corporation, Redmond, WA) to illustrate the emergence of resistance patterns over time globally, in Asia, and in Africa. Intervals of 5 years were chosen for histograms to produce a more detailed time series than every 10 years. Maps were created using an online open-source map tool.33,34 In keeping with the aim to aid country-based decisions on TCV introduction and guide empiric management of typhoid fever, the decision to not perform a meta-analysis was made to avoid pooling data of multiple drugs from multiple countries. As a secondary analysis of published data, this study was exempt from institutional review board approval.
RESULTS.
Our search of PubMed and Web of Science returned 6,724 and 3,949 articles, respectively (Figure 1). When including the references of relevant systematic reviews and then removing duplicates, we screened 7,047 titles and abstracts. Of these, 624 (8.9%) full-text articles were eligible for further review. We excluded 426 articles. The most common reason for article exclusion was failure to distinguish isolates that were collected from normally sterile sites from other sites, or the site was unspecified, resulting in 198 articles eligible for analysis (Supplemental Table S2
[ Typhoid fever might be rare in developed countries, but this ancient threat, thought to have been around for millennia, is still very much a danger in our modern world.
According to new research, the bacterium that causes typhoid fever is evolving extensive drug resistance, and it’s rapidly replacing strains that aren’t resistant.
Currently, antibiotics are the only way to effectively treat typhoid, which is caused by the bacterium Salmonella enterica serovar Typhi (S Typhi). Yet over the past three decades, the bacterium’s resistance to oral antibiotics has been growing and spreading. ]
Salmonella enterica serotype typhi is usually contracted by ingestion of food or water that is contaminated with the excrements of people that carry the organism and must survive the gastric pH barrier in the stomach prior to adherence in the small intestine. An infectious dose of Salmonella enterica serotype typhi in healthy individuals ranges between 1000 and 1 million organisms but can be related to the host’s defense mechanisms.
Salmonella enterica serotype typhi enter the submucosal region of the small bowel by either direct penetration into the epithelial tissue mediated by the cystic fibrosis transmembrane conductance regulator (CFTR) or via the M-cell, a specialized lymphoid epithelial cell. Once within the submucosa, the bacterium causes hypertrophy of the Peyer’s patches.
Dissemination of the organism from the Peyer’s patches occurs via the lymphatic system and the bloodstream. Cellular replication within the reticuloendothelial system is a hallmark of the disease and eventually causes the systemic symptoms that a clinician will observe. Following replication, organisms will reside in the macrophages of the liver, spleen, and bone marrow. Classically, Salmonella enterica serotype typhi can be cultured from the bone marrow even after anti-microbial therapy has been initiated.
Approximately 1% to 5% of patients will become chronic carriers of Salmonella enterica serotype typhi despite adequate antimicrobial therapy. A chronic carrier is defined as a patient that has excretion of the bacterium in the stool or urine for greater than 12 months after an acute infection and is typically of the female gender or has cholelithiasis. Those in the chronic carrier state will typically have high levels of antibodies to the Vi antigen and will not develop the clinical disease. The most famous of these chronic carriers was Mary Mallon who was diagnosed as a “healthy carrier” of the disease in 1906 after transmitting the disease to several households in which she served as the cook. The term “Typhoid Mary” became prominent during public health campaigns and is still used in modern culture today.

Of the 198 studies, 130 (65.7%) reported AST using CLSI interpretive criteria (Table 1). Among studies using CLSI criteria, 82 (63.1%) were before the 2012 breakpoint changes for fluoroquinolones.35 Ten (5.1%) studies used a combination of two AST interpretive criteria, and 59 (29.8%) studies did not report which AST interpretive criteria were used. Regarding laboratory antimicrobial susceptibility methods and findings, 173 (87.4%) of 198 studies used a disc diffusion method (e.g., the Kirby–Bauer test, Stokes’ method), whereas 82 (41.1%) used outputs from MIC techniques (e.g., broth micro-dilution, E-test, agar dilution) to determine resistant, intermediate, and susceptible isolates. Twelve (6.1%) used automated methods; 78 (39.4%) reported using a combination of a disc diffusion, MIC, or automated method; and nine (4.5%) did not report how susceptibility was determined.



Overall AMR.
Among all Salmonella Typhi isolates, 9,056 (25.9%) of 34,996 were resistant to chloramphenicol, 13,481 (38.8%) of 34,783 to ampicillin, and 13,366 (37.9%) of 35,270 to trimethoprim–sulfamethoxazole (Table 2). Of isolates, 12,666 (35.5%) of 35,659 were MDR, 9,495 (64.7%) of 14,671 were nalidixic acid resistant, and 5,406 (15.0%) and 6,979 (19.4%) of 35,975 were ciprofloxacin resistant and intermediate, respectively. Of isolates, 450 (1.3%) of 35,302 were resistant to ceftriaxone and 270 (4.5%) of 6,043 to azithromycin.



From 1990 through 1994, 955 (77.0%) of 1,241, 793 (73.6%) of 1,077, and 871 (79.3%) of 1,098 Salmonella Typhi isolates were resistant to chloramphenicol, ampicillin, and trimethoprim–sulfamethoxazole, respectively (Figure 3A). During the same period from 1990 through 1994, 1,205 (44.3%) of 2,719 were MDR. Of isolates from 2010 through 2014, 5,981 (44.6%) of 13,416 were MDR, and from 2015 through 2018 1,679 (32.7%) of 5,140 were MDR. Of isolates in the time periods 2005–2009, 2010–2014, and 2015–2018, 27 (2.1%) of 1,279, 93 (4.1%) of 2,263, and 150 (6.7%) of 2,247 were resistant to azithromycin, respectively.

(A) Antimicrobial resistant Salmonella Typhi isolates worldwide, 1972–2018. (B) Antimicrobial resistant Salmonella Typhi isolates in Asia, 1972–2018. (C) Antimicrobial resistant Salmonella Typhi isolates in Africa, 1972–2018. Full data provided in Supplement Table S4.
Ordered chronologically by antimicrobial agent introduction and grouped by color by multidrug resistant and extensively drug resistant phenotypes. †Fluoroquinolone includes ciprofloxacin and ofloxacin.
Third-generation cephalosporin includes ceftriaxone and cefotaxime.
Antimicrobial resistance in Asia.
When stratified by time periods 1972–1989, 1990–1999, 2000–2009, and 2010–2018 in the Asia region, the median (interquartile range) proportion of Salmonella Typhi isolates that were MDR was 0.0% (0.0%), 31.2% (22.9–47.0%), 16.2% (6.1–35.6%), and 5.5% (2.0–24.3%), respectively (Table 3). By time period, ciprofloxacin resistance was found in zero (0.0%) of 61, 219 (3.7%) of 5,912, 439 (3.1%) of 14,040, and 4,670 (41.1%) of 11,349 (χ2 5,376, P < 0.001) isolates. By time period, ceftriaxone resistance was found in zero (0.0%) of 203, 124 (2.5%) of 4,898, 47 (0.4%) of 12,761, and 266 (1.9%) of 13,970 (χ2 2.3, P = 0.133) isolates.




Of isolates from 2015 through 2018, 1,638 (32.6%) of 5,032 were MDR, 167 (5.7%) of 2,914 were resistant to third-generation cephalosporins, 148 (8.3%) of 1,777 to azithromycin, and 20 (3.4%) of 594 to meropenem (Figure 3B). Two studies from Pakistan reported 14 (2.6%) of 546 isolates were XDR.36,37
Antimicrobial resistance in Africa.
Two studies tested 3,327 isolates during the time period 1972 through 1989, and neither study reported testing trimethoprim–sulfamethoxazole, MDR, ciprofloxacin, ceftriaxone, or azithromycin (Table 4).38,39 In the time periods 1990–1999, 2000–2009, and 2010–2018, the median (interquartile range) proportion of MDR Salmonella Typhi isolates was 0.0% (0.0%), 0.0% (0.0–25.5%), and 38.0% (30.4–85.7%), respectively. Of isolates during the same three time periods, ciprofloxacin resistance was found in zero (0.0%) of 133, 14 (1.2%) of 1,209, and 39 (1.2%) of 3,228 (χ2 0.7, P = 0.415), respectively. Of isolates, ceftriaxone resistance was found in zero (0.0%) of 55, eight (0.7%) of 1,160, and five (0.2%) of 2,212 (χ2 2.9, P = 0.09), respectively. No eligible studies in Africa reported azithromycin resistance until the 2010–2018 period. Of isolates in 2010–2018, five (0.5%) of 954 were azithromycin resistant. One study reported zero (0.0%) of seven isolates resistant to meropenem in 2013.


Among studies reporting MDR isolates, one study reported zero (0.0%) of 37 MDR isolates from 1995 through 1999.41 Of isolates during the periods 2000–2004, 2005–2009, and 2010–2014, 28 (21.9%) of 128, 198 (21.2%) of 932, and 2,132 (76.5%) of 2,787 isolates were MDR, respectively (Figure 3C). From 2015 through 2018, one study in Democratic Republic of the Congo reported 41 (38.0%) of 108 isolates were MDR.42 Among isolates from 2015 through 2018, 357 (60.6%) of 589 were resistant to chloramphenicol, 343 (70.9%) of 484 to ampicillin, and 396 (69.4%) of 571 to trimethoprim–sulfamethoxazole. Third-generation cephalosporin resistance was found in 35 (29.4%) of 119, 24 (9.2%) of 262, 13 (1.2%) of 1,111, four (0.2%) of 2,416, and one (0.9%) of 111 in 1995–1999, 2000–2004, 2005–2009, 2010–2014, and 2015–2018, respectively. No eligible studies from Africa reported XDR isolates.
Other typhoidal and non-typhoidal Salmonella.
Among 12,850 other typhoidal Salmonella isolates tested, 10,464 (81.4%) were Salmonella serovar Paratyphi A, 1,305 (10.2%) Salmonella Paratyphi A or Paratyphi B, 1,012 (7.9%) unspecified Salmonella “Paratyphi,” 68 (0.5%) Salmonella Paratyphi B, and one (< 0.1%) Salmonella Paratyphi C. Of 1,462 non-typhoidal S. enterica isolates tested, 793 (54.2%) were Salmonella Typhimurium and 669 (45.8%) were Salmonella Enteritidis. Of Salmonella Paratyphi A isolates, 650 (8.9%) of 7,335 were MDR, 3,027 (32.4%) of 9,332 were resistant to fluoroquinolones, and 45 (2.1%) of 2,184 were resistant to azithromycin. Antimicrobial susceptibility testing data for typhoidal Salmonella other than serovar Typhi are presented in Supplemental Table S4.
DISCUSSION.
We demonstrate that AMR among Salmonella Typhi isolates is a substantial problem in countries in Asia and Africa. Multidrug resistant Salmonella Typhi remains prevalent in Asia, with resistance developing to an increasing number of antimicrobial classes such that XDR Salmonella Typhi is now a major threat. MDR Salmonella Typhi is a growing problem in Africa.
The first AMR phenotype to appear in our review was resistance to chloramphenicol in a study from Vietnam in 1972.43 We show clear evidence of increasing prevalence of resistance to traditional first-line antimicrobials in the 1980s and a substantial increased prevalence of MDR in the 1990s. Because third-generation cephalosporins and azithromycin were not widely used or available for the treatment of typhoid fever from 1970 through 1989,7,44 data were lacking on susceptibility to these drugs during earlier time periods.
When stratified by region, resistance to the three traditional first-line antimicrobials and MDR appear later in Africa compared with Asia. This difference is consistent with phylogenetic analyses of whole-genome sequencing data, suggesting the introduction of the MDR H58 haplotype from Asia to Africa.45–47 As there were no eligible studies located in Oceania, we could not address AMR in this region. The H58 haplotype was identified in Fiji as early as 1992.45 However, the H58 haplotype has so far not expanded in Fiji where most Salmonella Typhi isolates remain susceptible to traditional first-line antimicrobials.48,49 We observed a decline in the median prevalence of resistance to each of the traditional first-line antimicrobials and in MDR across Asia, corroborating reports of increasing prevalence of chloramphenicol-susceptible strains in areas that previously documented a high prevalence of resistance to the drug.
The trend of resistance to a growing number of antimicrobial classes is alarming, including recently to azithromycin37,54,55 and outbreaks of XDR Salmonella Typhi.12–14 Our review captured one study in Pakistan36 and one in Indonesia56 reporting meropenem resistance in Salmonella Typhi. To our knowledge, these would be the first reports of carbapenem resistance in Salmonella Typhi and cause for great concern. We recommend that this finding be confirmed with additional testing of the isolates. There were no eligible articles in our review reporting XDR Salmonella Typhi from Africa. However, if the history of the spread of MDR Salmonella Typhi applies, XDR Salmonella Typhi is likely to be introduced and spread in Africa in due course. Resistance to multiple antimicrobial classes is likely being driven by indiscriminate antimicrobial use, and weak stewardship practices in the community and in healthcare facilities.
Because we sought to produce a comprehensive review of AMR to assist countries with decision-making about TCV introduction and to guide empiric management decisions, we decided a priori against conducting a meta-analysis that would produce pooled prevalence estimates. Furthermore, because the overwhelming majority of eligible studies were located in Southern Asia and reported a broad range of antimicrobials, pooled estimate would be of little value when evaluating AMR in Salmonella Typhi for a specific country that was not part of the pooled analysis.
An earlier systematic review and meta-analysis of enteric fever produced pooled estimates for MDR and fluoroquinolone resistance.58 The earlier review and ours both demonstrate that although data are limited for known typhoid-endemic areas, antimicrobial resistant Salmonella Typhi is becoming more prevalent. However, our review also had a number of additional strengths. First, Browne and others classified intermediate organisms as resistant. According to the CLSI, the intermediate category “implies clinical efficacy in anatomical sites where the drugs are physiologically concentrated” and the resistant category “implies clinical efficacy of the agent against the isolate has not been reliably shown in treatment studies.”59 In keeping with this guidance, we did not categorize intermediate as a category of resistant isolates, and thus avoided possible bias toward inflation in the number of resistant isolates. Second, we classified isolates as MDR if the study authors clearly defined MDR isolates as resistant to chloramphenicol, ampicillin, and trimethoprim–sulfamethoxazole, and we could ascertain that resistance to these three first-line antimicrobials was present. Third, we placed no restrictions on the number of isolates the study tested for resistance. Fourth, we required studies to report the dates for data collection. If a study did not report dates, it was excluded, and we did not impute dates based on study publication date. By not pooling the proportions, recategorizing intermediate isolates, or imputing data, we believe our review presents raw data that are readily accessible to decision-makers.
Our study had a number of limitations. First, a substantial proportion of included studies did not report the interpretive criteria used, and we were unable to make adjustments to the interpretive criteria based on the current CLSI or other breakpoint guidelines because we did not have access to zone sizes or MIC values for most studies. Notably, the CLSI interpretive criteria for Salmonella Typhi have changed over time, including to fluoroquinolones, third-generation cephalosporins, and the introduction of azalide break points. These changes may have generated artefactual variation in the prevalence of resistance over time. Second, without having a full classification of susceptible, intermediate, and resistant isolates in every study, we were also limited by having to impute data on resistant isolates in studies that only reported those that were susceptible or that only provided the proportion and total number of isolates tested. Third, our data comprised mostly hospital and healthcare facility–based studies that may overrepresent AMR. Finally, our global AMR data are driven by the predominance of studies located in Asia, particularly India, Nepal, and Pakistan. Several UN regions and subregions had no eligible studies or were underrepresented. Higher income countries in Northern America and Northern, Southern, and Western Europe usually rely on national surveillance systems to report AMR.60,61 No eligible studies were identified from Oceania, Central America, Caribbean, or Eastern Europe. Although studies were included from South America, Northern, Middle, and Southern Africa, and Eastern, Central, and Western Asia, these were limited in number and dominated by studies in Eastern Africa, and Southeastern and Southern Asia.
The prevalence of resistance among Salmonella Typhi isolates is growing, especially the XDR phenotype in Asia and the MDR phenotype in Africa. Isolates resistant to many classes of antimicrobials pose a substantial threat to global health. Typhoid control efforts should be expanded, including the introduction of TCV which has been demonstrated to reduce typhoid fever incidence in endemic areas62 and was recommended to combat and control XDR.63 Where XDR Salmonella Typhi is present, azithromycin and carbapenems remain effective for uncomplicated and complicated typhoid fever, respectively. We encourage the implementation of robust stewardship and surveillance programs to inform empiric treatment decisions and reduce AMR.
Acknowledgments.
We would like to thank Ariella P. Dale for her contribution to screening full text and extracting study characteristics, and Chuen Yen Hong for translating articles in Chinese text.
Am J Trop Med Hyg. 2020 Sept. 28;103(6):2518–2527. doi: 10.4269/ajtmh.20-0258.
PMC Copyright notice.
PMCID: PMC7695120 PMID: 32996447.
© The American Society of Tropical Medicine and Hygiene.
Address correspondence to John A. Crump, Centre for International Health, 55 Hanover Street, University of Otago, Dunedin Central, Dunedin 9016, New Zealand. E-mail: john.crump@otago.ac.nz
Authors’ addresses: Christian S. Marchello, Samuel D. Carr, and John A. Crump, Centre for International Health, University of Otago, Dunedin Central, Dunedin, New Zealand, E-mails: christian.marchello@otago.ac.nz, sam.carr@otago.ac.nz, and john.crump@otago.ac.nz.
Corresponding author..
As a library, NLM provides access to scientific literature. Inclusion in an NLM database does not imply endorsement of, or agreement with, the contents by NLM or the National Institutes of Health.
Learn more: PMC Disclaimer | PMC Copyright Notice
The American Journal of Tropical Medicine and Hygiene logo
Am J Trop Med Hyg. 2020 Sep 28;103(6):2518–2527. doi: 10.4269/ajtmh.20-0258
.
.
.
.
.