June 28, 2022.
The studies used viruses that specialize in killing bacteria, illustrated above, to treat multidrug-resistant bacteria in patients’ lungs. MattLphotography / Shutterstock.
Bacteria with resistance to multiple antibiotics are a growing problem worldwide. As a result, some types of infections are becoming increasingly difficult to treat, especially in healthcare facilities and in people with weakened immune systems.
In addition to developing novel antibiotics, researchers have been exploring other ways to treat drug-resistant bacteria. One experimental technique is the use of bacteriophages, also called phages. Phages are viruses that infect only bacteria and so are harmless to people.
Previously, a team led by Dr. Graham Hatfull from the University of Pittsburgh engineered phages to be more efficient at killing bacterial cells.
These were successfully used to treat a teenager with a life-threatening antibiotic-resistant infection after a lung transplant. The teen required drugs to suppress her immune system because of the transplant. This immunosuppression prevented her immune system from making antibodies that might have neutralized the phages before they killed the bacteria.
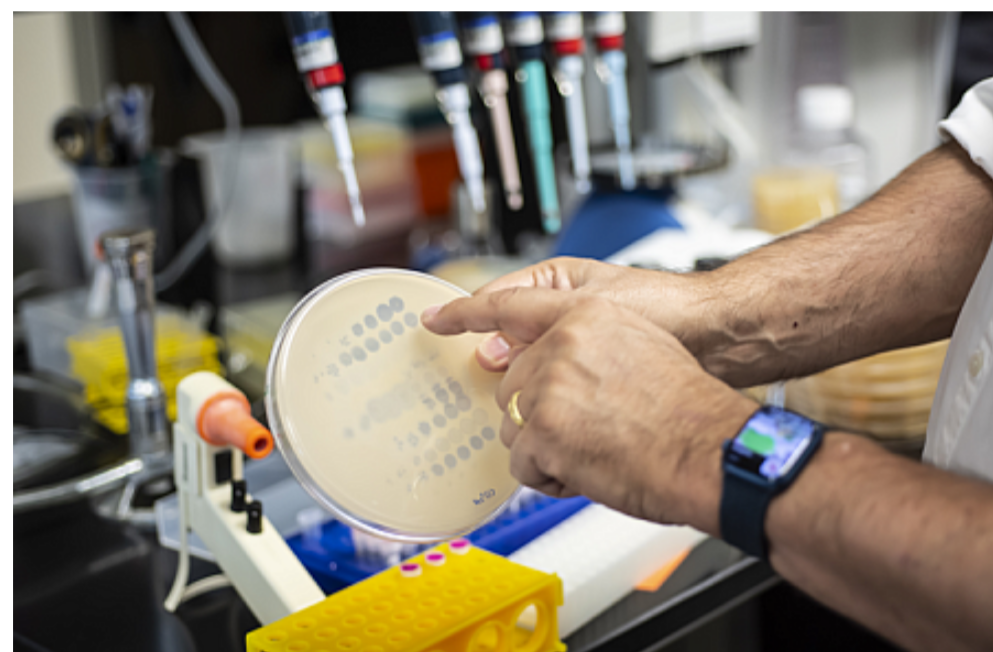
In a new case study, researchers led by Drs. Jerry Nick and Rebecca Davidson from National Jewish Health tested phage therapy in a 26-year-old man with advanced cystic fibrosis and a severe, multidrug-resistant Mycobacterium abscessus lung infection. Hatfull’s group screened a panel of phages for candidates that could kill the specific strain of M. abscessus infecting the patient.
The patient received twice-daily infusions of the engineered phages along with antibiotics. Results from the study, which was funded in part by NIH, were published on May 26, 2022, in Cell.
After about a year of phage therapy, there was no evidence of ongoing M. abscessus infection in cultured lung samples. By the eighth month of treatment, the patient’s immune system had recognized and produced antibodies capable of neutralizing one of the phages.
However, the other remained active.
With his M. abscessus infection cleared, the patient underwent a successful lung transplant. The team found no evidence of M. abscessus in the removed lungs or in the new lungs several months after transplant. The patient remained on phage therapy at the time the results were published at 500 days of treatment.
He has since been able to stop taking both antibiotics and phage.
In another study, an international team led by Hatfull provided phage therapy for compassionate use in 20 people with life-threatening antibiotic-resistant infections. Most of the patients had cystic fibrosis and M. abscessus infections. For 11 of them, only a single type of phage was found that could likely kill their specific bacteria. For the nine others, the researchers identified two or more potentially useful phages.
The patients received their phages twice daily, either into a vein or inhaled. Results from this case series, which was also funded in part by NIH, were published on June 9, 2022, in Clinical Infectious Diseases.
Of the 20 volunteers, five experienced total or substantial resolution of their infection. Of these, two were able to undergo lung transplantation. Another six patients had partial responses to phage therapy. Five additional patients either had short-lived or inconclusive improvements in infection. In four, there was no detected improvement in response to the phage therapy.
None of the patients experienced serious side effects from the treatment. Some of their immune systems generated antibodies against one or more of the phages. However, despite this immune reaction, the phage treatment appeared successful in most of these cases, even when only a single type of phage was used.
These studies highlight the potential of phage therapy as a method of personalized, precision treatment for severe antibiotic-resistant infections. More work is needed to optimize phage delivery and prevent the immune system from neutralizing the phages. Additional phages that can kill more types of bacteria are also required.
“We’ve not yet figured out how to find or engineer phages that will get every strain of bacteria in these patients,” Hatfull notes. “That represents one of the major challenges ahead.”
By Sharon Reynolds.
Source, NIH, Bethesda, USA.